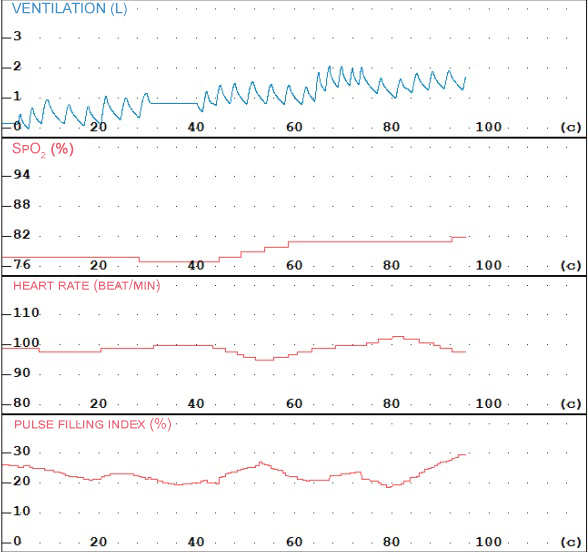
 In the Pulse oximetry mode, MAS2 spirometers record saturation (SpO2), heart rate (HR) and pulse waveform – photoplethysmogram.
In the Pulse oximetry mode, MAS2 spirometers record saturation (SpO2), heart rate (HR) and pulse waveform – photoplethysmogram.
SpO2 and heart rate values are reflected in the standard protocol for spirometric studies on MAS2.
Indications for computerized pulse oximetry are: obesity level 2 and above (body mass index >35), arterial hypertension grade 2 and above, severe COPD (FEV1 <50%), heart failure of functional class II and above, respiratory failure grade 2 and higher, cor pulmonale, metabolic syndrome, Pickwick syndrome, hypothyroidism, snoring and sleep apnea followed by snoring, frequent nighttime urination (>2 times per night), shortness of breath, shortness of breath or choking attacks at night, night sweats, frequent awakenings and unrefreshing sleep, fatigue in the morning, morning headaches, cyanosis, severe daytime sleepiness, depression, apathy, irritability, decreased mood background, gastroesophageal reflux at night, dynamic monitoring of the effectiveness of respiratory support methods – long-term oxygen therapy using oxygen concentrators, non-invasive auxiliary ventilation of the lungs with constant positive pressure (CPAP therapy) and two-level positive pressure (BiLevel therapy).
Pulse oximetry is also necessary for solving expert questions in a number of diseases leading to the development of chronic respiratory failure (CRF) to objectify the degree of the latter. Known clinical criteria for CRF (respiratory rate, HF, exercise tolerance, etc.), including the indicators of the study of respiratory function. However, due to compensatory mechanisms against the background of a long period of time of CRF development, clinical criteria may not always reflect its true severity. To objectify the degree of respiratory failure, it is necessary to use blood gas analysis. So, for RF I degree, SpO2 93-98% and the corresponding indicators of PaO2 80-100 mm Hg are characteristic, RF II degree corresponds to a decrease in saturation – SpO2 86-92%, which corresponds to PaO2 75-85 mm Hg at rest in the absence of hypercapnia (PaCO2 35-45 mm Hg) in both stages. With III degree RF, hypercapnia develops (PaCO2 more than 45 mm Hg) against the background of a further decrease in saturation – less than 85% and PaO2 less than 75 mm Hg.